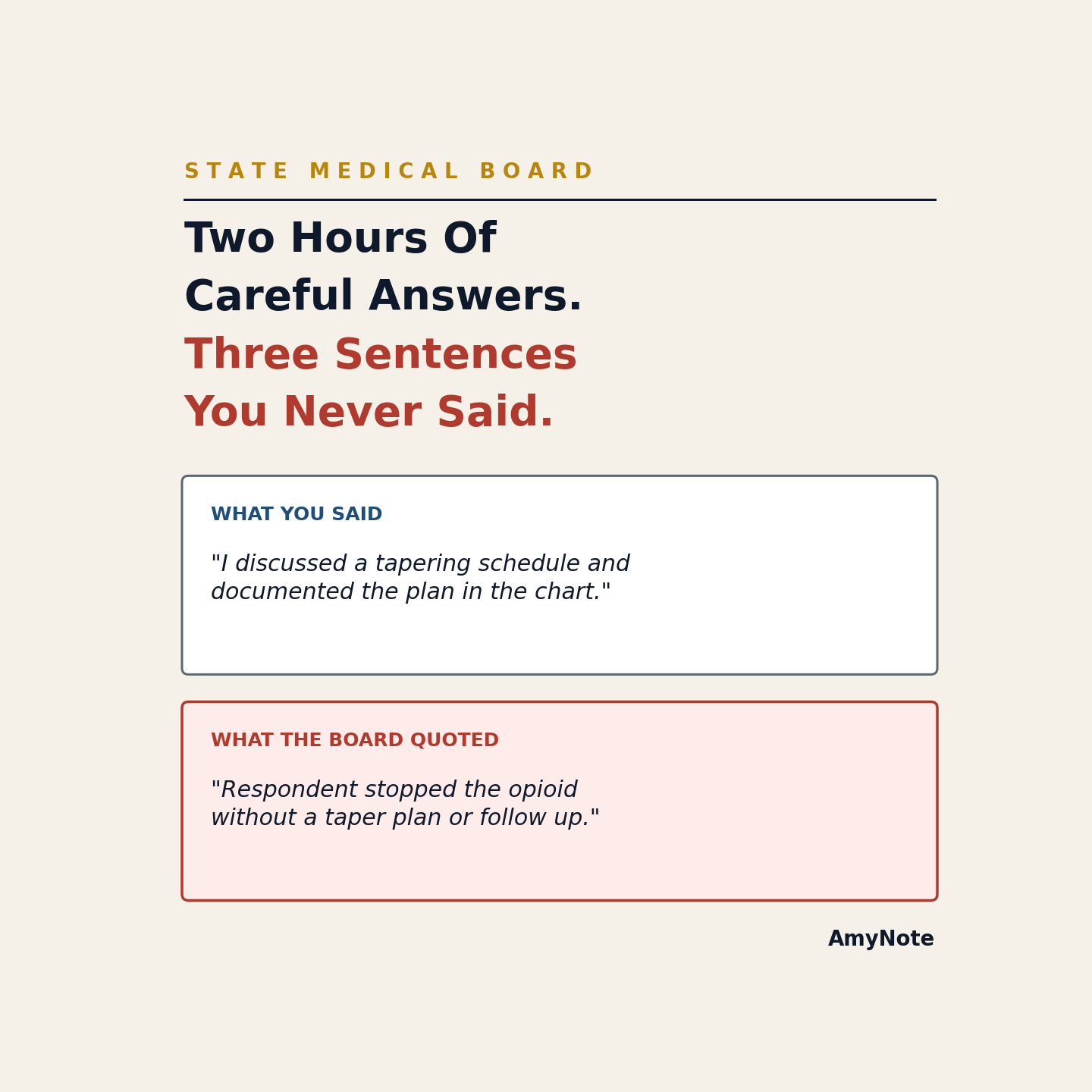
The investigator closes her binder at 4:20 PM after nearly two hours of questions about your 2024 chart notes for Patient K.L. You walk her to the parking lot, drive back to clinic, and by the time you sit down for your next patient you cannot remember whether you told her the differential included pulmonary embolism or only community-acquired pneumonia. Eight months later the Statement of Charges quotes you from her Report of Investigation, and the quote is not what you said.
The Problem
State medical boards run a subject interview that has no court reporter and no recording. Under most state Medical Practice Acts, once a complaint moves from screening to formal investigation, the board investigator schedules an interview with the physician of record. Those meetings are handwritten or laptop-typed and are not transcribed. The investigator leaves with a notebook, drafts a Report of Investigation over the next several weeks, and that ROI becomes the internal file that decides whether to refer the matter for probable cause.
The record that matters is the investigator's synthesis, not the words the physician actually said. When the Statement of Charges arrives, often six to nine months after the interview, it cites conversations no one can quote back. The physician has to reconstruct clinical reasoning about a specific patient encounter, the differential diagnosis considered, the timing of the disposition decision, and whether the chart documentation kept pace with the reasoning explained in the room.
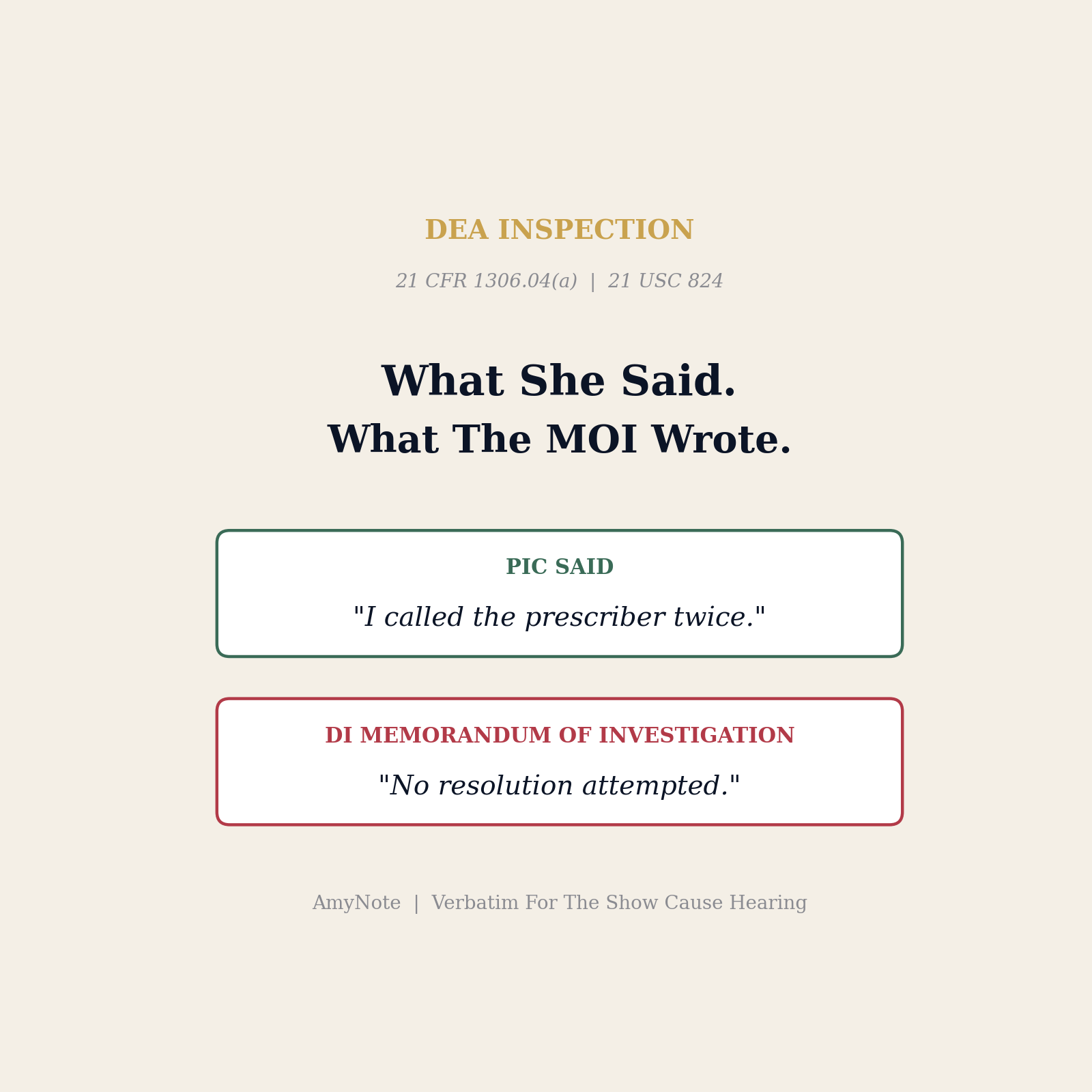
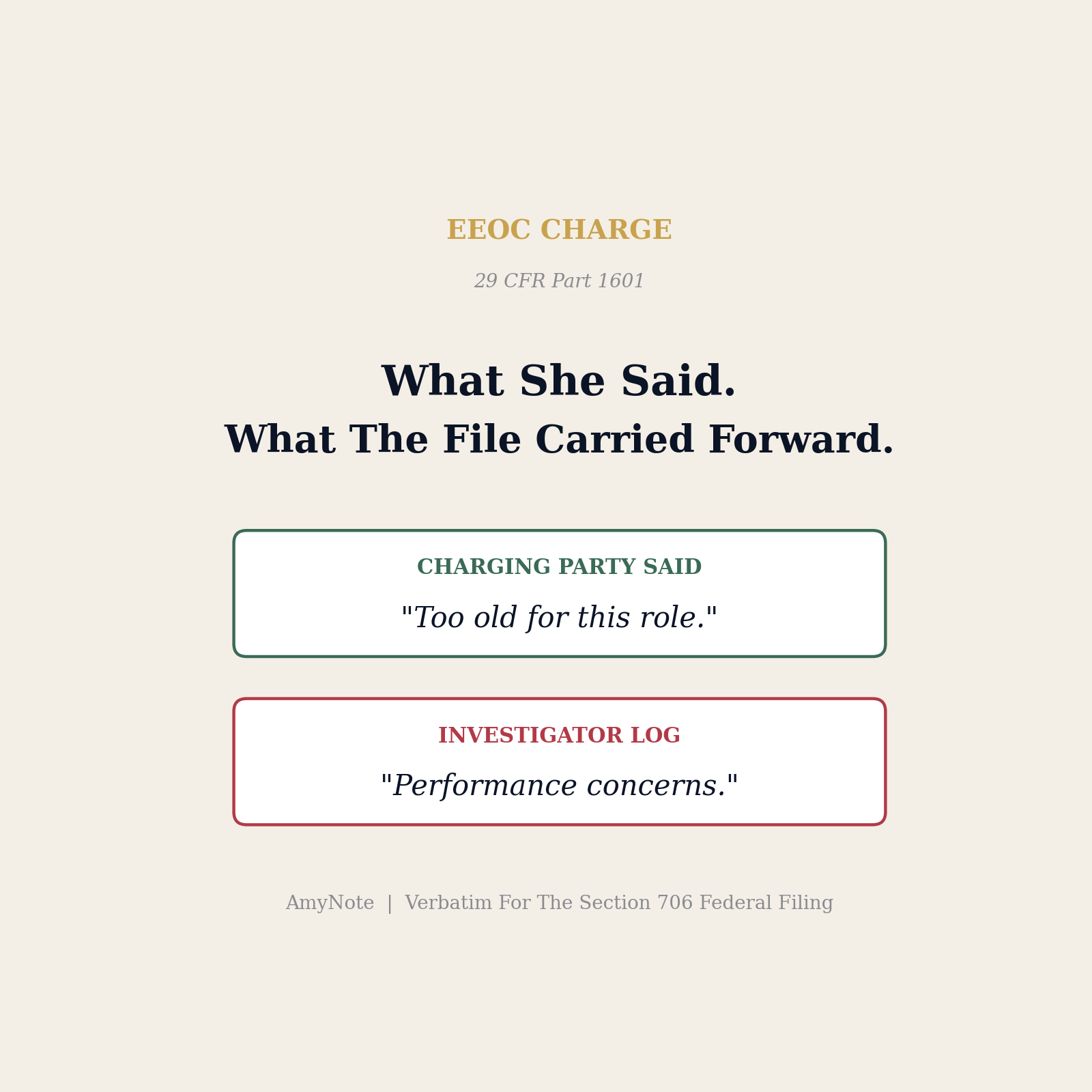
Physicians then face a short answer window that combines a factual denial, a legal defense, and a remediation posture. Counsel is asked to attest to statements that live only in the investigator's notebook. The interview is the evidence, and no one owns the evidence. Every physician who has been through an ROI gap describes the same experience: the paraphrase in the Report reads like a clinical error the physician never confessed to, and there is no way to prove what was actually said in the room.
Why Current Solutions Fail
Bringing counsel to take notes sounds useful and rarely works. Counsel is triaging privilege, tracking prior statements against the chart, and cannot write full sentences while the physician answers a follow-up about the timing of a repeat troponin. Every defense attorney who has taken these notes will admit the transcript is a paraphrase at best. The disagreements at the interview do not survive into a legal pad; the nuances are exactly what the ROI later drops.
The other habit is a debrief memo drafted the same afternoon. Debrief memos capture the physician's version of the conversation, not the investigator's. When the ROI cites a phrase the physician does not remember using, the memo cannot rebut it. Counsel then argues interpretation, not fact. Interpretation loses to a written record almost every time.
A third habit is to rely on the fact that the board investigator might have their own recording. In practice, investigator recordings are variable, are treated as internal work product, and are not automatically produced to counsel during discovery. Even in states where the recording is later disclosed, the timing is wrong: the physician needs the transcript before the Answer to the Statement of Charges is due, not after depositions have started.
What Actually Works
Capture the full audio of the interview and hold a searchable transcript from the moment the investigator closes the door. Most state Medical Practice Acts permit the physician to record with consent or written notice, and the board investigator will usually agree on the record. Fourteen U.S. states are one-party-consent jurisdictions, which permits the physician to record without asking. In two-party-consent states, a clear on-the-record notice at the start of the interview satisfies the statute. With that consent, the physician or defense counsel runs AmyNote on a phone during the interview.
AmyNote uses the OpenAI Speech API for high-accuracy multi-speaker transcription and Anthropic Claude Opus for structured summaries. The transcript is timestamped, the summary is written against the clinical vocabulary of the encounter, and both are ready before the physician gets back to clinic. There is no bot in the room and no participant to explain. The physician's phone sits on the table like a phone; the app captures the audio, and the transcript lands on the physician's device before the drive home is over.
Every subsequent step gets faster. Counsel reviews the transcript for accuracy that same evening. Board investigator paraphrases can be checked against the exact words spoken. When the ROI arrives eight months later, the response team can pull the exact question and the exact answer next to the investigator's paraphrase. The defense stops arguing about what the physician meant and starts citing verbatim testimony.
Privacy is a boundary condition, not a footnote. Both OpenAI and Anthropic contractually guarantee zero training on user data. Audio is encrypted in transit and is not retained after processing. Transcripts are stored locally on the device with end-to-end encryption. That posture is compatible with HIPAA minimum-necessary standards, state licensing confidentiality rules, and the attorney-client privilege that attaches to interview preparation.
The gap closes when the physician owns the words. Charges get withdrawn or amended. Consent orders shift toward continuing education and away from license restrictions. Answers to a Statement of Charges cite documented behavior instead of hypothetical process failures. The physician gets to walk into every subsequent hearing knowing that the record is the record, not the investigator's paraphrase of it.
A Practical Playbook For Defense Counsel
The workflow that consistently closes the ROI gap looks the same across states:
- Install AmyNote on the physician's phone before the interview date is confirmed. Give the physician one or two low-stakes sessions to get comfortable with tapping record and confirming the summary. A hospital peer review or credentialing meeting is a good pilot.
- Confirm the consent posture in the physician's state. In one-party consent states, no notice is required. In two-party states, a scripted on-the-record consent line at the start of the interview satisfies the statute; the investigator's verbal agreement lives in the recording itself.
- Start capture at the greeting. Do not wait for the substantive questions to begin. The framing sentences, the investigator's characterization of the complaint, and the introductions all matter later when the ROI narrative arrives.
- Route the transcript to counsel the same evening. Use secure sharing, not email attachments. Counsel reviews the summary against the chart that night and flags any statement that the ROI could paraphrase against the physician.
- Cross-reference against the ROI when it lands. Pull the exact investigator question and the exact physician answer next to the ROI paraphrase. The Answer to the Statement of Charges cites the transcript, not the memory of the interview.
Getting Started
Install AmyNote on the physician's phone before the board investigator confirms an interview date. Pilot it in one hospital peer review or credentialing session so the physician is fluent with the workflow before the state investigator arrives. When the interview starts, obtain consent on the record, begin capture at the greeting, keep it running through the closing, and route the transcript to defense counsel the same evening. The next Answer you file will be shorter, sharper, and built on evidence rather than recall.
Try AmyNote free for three days at amynote.app, no credit card required. Whatever the next investigator's binder looks like, the physician's transcript should already exist.
Originally published as an X Article by @AmyNoteApp.